You just brought a tiny human home. Nothing in life fully prepares you for those first days — the wonder, the terror, the three-hour feeding cycles at 2 AM, the frantic Googling at 4 AM. This guide is everything your Babynama pediatrician would tell you if you had an hour with them. It is written for Indian parents, with Indian realities in mind.
Quick Answer: First Week Checklist
What your newborn needs in the first week:
- Feed 8–12 times per day — every 2–3 hours, including at night. Do not let a newborn sleep more than 3–4 hours without a feed in the first two weeks.
- Watch for jaundice — yellowing of skin and eyes. Mild jaundice on day 2–3 is normal; yellow color reaching the belly or below the knees needs a doctor visit same day.
- Keep the cord stump dry — fold the diaper down, no water or oil on the stump until it falls off.
- Sponge bath only until the cord falls off (7–21 days). No full immersion bath until then.
- Skin-to-skin contact as much as possible — for bonding, warmth, and breastfeeding success.
- Watch for wet diapers — at least 6 per day by day 5 tells you baby is getting enough milk.
- Vitamin K injection at birth — do not skip this.
- First vaccines at birth — BCG, OPV-0, Hepatitis B. More at 6 weeks.
- ⚠️ In a baby under 3 months, ANY fever of 100.4°F (38°C) or higher is a medical emergency — see a doctor the same day, even at night. Do not give paracetamol and wait.
- Sleep on back, always.
The First Hour After Birth
The first hour after birth is sometimes called the “golden hour” — and for good reason. This is when several things should happen that have lasting benefits for your baby.
Skin-to-Skin Contact
The moment your baby is born and breathing well, she should be placed directly on your bare chest. This is true whether you had a vaginal delivery or a C-section — most hospitals in India now support skin-to-skin even after surgical births. This contact does several things at once: it regulates your baby’s body temperature better than any warmer, stabilizes her blood sugar, lowers her cortisol levels, and triggers the hormones in you (oxytocin) that kick-start bonding and milk production. Try to keep skin-to-skin uninterrupted for at least one hour.
Delayed Cord Clamping
If your delivery is uncomplicated, ask your doctor or midwife to wait at least 1–3 minutes before clamping the umbilical cord. During this time, blood from the placenta continues flowing into your baby — an estimated 80–100 ml of blood that contains iron stores that protect against anemia for the first 6 months of life. This is especially important for babies born in settings where iron deficiency is common. Most Indian hospitals are now aware of this practice; it is worth mentioning in your birth plan.
The First Breastfeed
Your baby has a strong sucking reflex at birth and is most alert in the first hour of life. This is the ideal time for the first breastfeed. What comes out of your breast in these first days is not “real milk” yet — it is colostrum, and it is the most valuable thing you can give your baby. More on this in the feeding section below.
Vitamin K Injection
Every newborn receives a Vitamin K injection at birth — or should. This is one of the few genuinely non-negotiable interventions in newborn care. Babies are born with almost no Vitamin K stores, and without it, they are at risk of a rare but devastating condition called Vitamin K Deficiency Bleeding (VKDB), which can cause internal bleeding including in the brain. The injection is safe, effective, and gives protection for weeks. There are oral drops available, but the injection is significantly more reliable. If anyone tells you to skip this or offers “herbal alternatives,” the answer is no.
Eye Drops (Erythromycin Prophylaxis)
In many hospitals, antibiotic eye drops or ointment are applied to the newborn’s eyes shortly after birth to prevent infection from bacteria that can be present in the birth canal. This is standard practice. The drops may cause mild, temporary blurring of vision — which is why the golden hour of skin-to-skin is recommended before they are applied when possible.
Newborn Appearance: What’s Normal (and What Surprises New Parents)
Your baby may not look the way you expected. Here is what is usually normal, even if it looks alarming.
Vernix Caseosa
A white, waxy coating on the skin at birth. It is not dirt — it is a protective layer that has been keeping your baby’s skin safe in the womb. There is no need to wash it off immediately. In fact, leaving it on for a few hours allows the skin to absorb it. It has natural antimicrobial properties.
Lanugo
Fine, soft hair covering the body — particularly visible on the shoulders, back, and face. More common in premature babies. It sheds on its own within a few weeks. Not a medical concern.
Moulded Head
If your baby was delivered vaginally, her head may look elongated, cone-shaped, or uneven. The skull bones overlap during passage through the birth canal. This resolves on its own within days.
Swollen Genitals
Both boys and girls often have swollen genitals at birth due to maternal hormones crossing the placenta. Girls may even have a small amount of vaginal discharge or spotting — this is a “mini period” caused by withdrawal from your estrogen and is usually normal. It resolves within a week or two. Heavy or persistent bleeding, however, is not — mention it to your pediatrician.
Milia
Tiny white bumps on the nose and cheeks. These are blocked sebaceous glands and are very common. Do not squeeze or treat them — they disappear on their own within a few weeks.
Newborn Acne
Red, pimple-like spots appearing around 2–4 weeks of age. Again caused by maternal hormones. It looks alarming, but needs no treatment. Do not apply creams, oil, or besan on it. It clears by 4–6 weeks.
Jaundice
Yellowing of the skin and whites of the eyes, typically appearing on day 2–3 of life. So common that it affects 60% of full-term newborns and 80% of premature babies. The causes and when to worry are covered in detail below.
Newborn Reflexes
Your newborn arrives pre-programmed with a set of automatic responses called primitive reflexes. These are not learned behaviors — they are hardwired at birth and serve important purposes.
Rooting reflex: Stroke your baby’s cheek or corner of the mouth and she will turn toward that side and open her mouth. This is how she finds the breast for feeding. It fades around 3–4 months as feeding becomes voluntary.
Sucking reflex: Touch the roof of her mouth and she sucks automatically. This is already well-developed — babies practice this in the womb from around 28 weeks. It works together with rooting for feeding.
Moro reflex (startle reflex): A sudden noise, movement, or sensation of falling causes the baby to fling arms wide, extend the neck, then bring the arms back together. Often followed by crying. This can look frightening to parents but is normal and expected. Swaddling helps reduce the frequency of Moro-triggered startles during sleep. It fades around 3–6 months.
Palmar grasp reflex: Place your finger in your baby’s palm and she will grip it firmly — often strongly enough that you think she is going to hold on forever. This reflex fades around 5–6 months and is replaced by intentional grasping.
Stepping reflex: Hold your baby upright with her feet touching a flat surface and she will make stepping motions as if trying to walk. This is not a sign of readiness to walk — it is a primitive reflex that disappears around 2 months, before returning as intentional stepping at around 8–12 months.
These reflexes matter clinically. A pediatrician checks them at birth and follow-up visits. The fade-out ages above are typical ranges, not fixed dates. Tell your pediatrician if a reflex is clearly present on one side but not the other, seems completely absent, or persists well beyond 6 months — asymmetric or persistent reflexes can signal neurological concerns, which is why routine check-ups in the first weeks are important.
Feeding Your Newborn
Colostrum: The First Milk
In the first 2–3 days, your breasts produce colostrum — small amounts (a teaspoon or two per feed) of thick, yellowish fluid. Do not be alarmed by the tiny quantity. Your baby’s stomach is the size of a marble on day one. Colostrum is extraordinarily concentrated: it is packed with antibodies (especially IgA, which coats the gut lining), white blood cells, and growth factors. It is also a laxative — it helps your baby pass meconium (the dark first stool), which in turn helps clear bilirubin and reduces jaundice. Colostrum cannot be replaced by formula. Feed as frequently as your baby demands, even if each session feels short.
Milk Coming In
Your mature milk comes in between days 2 and 5. Many mothers feel their breasts become suddenly full, warm, and firm — this is called engorgement. It can be uncomfortable. Feed frequently and on demand. Hot compresses before feeding help the milk flow; cold packs after feeding reduce swelling.
Feeding Frequency
8 to 12 times per day is the range for a newborn. That works out to roughly every 2–3 hours. Newborns cannot store much milk, their stomachs empty quickly, and breast milk is digested faster than formula. In the first 2 weeks especially, do not let your baby sleep more than 3–4 hours without a feed, even at night, until your pediatrician confirms weight gain is on track.
Signs Your Baby Is Getting Enough Milk
This is the number one anxiety for breastfeeding mothers in the first week, and understandably so — you cannot see how much milk the baby is taking.
Watch for these reassuring signs:
- At least 1–2 wet diapers on day 1, 2–3 on day 2, 4–5 on day 3, and 6+ per day from day 5 onward
- Dark meconium stools transitioning to yellow by days 3–5
- Active and alert when awake (not just sleepy)
- Audible swallowing during feeds
- Weight loss of less than 7–10% of birth weight in the first days, with return to birth weight by 10–14 days
Normal Newborn Weight Loss
Almost all newborns lose weight in the first few days. Up to 7% weight loss in a breastfed baby is considered normal; up to 10% is acceptable but worth monitoring closely. This is not a failure of breastfeeding — it is fluid shifting and meconium passing. Most babies regain birth weight by 10 days and continue gaining 20–30 grams per day after that.
Formula: If It Is Needed
If your baby is losing excessive weight, not producing enough wet diapers, or you have a genuine supply issue, formula supplementation is not a failure. Fed is what matters. If you do supplement, express breast milk at the same time to protect your supply. Consult your pediatrician before switching entirely to formula — many supply issues are temporary and solvable.
Breastfeeding Positions
Ensure a deep latch. Your baby’s mouth should cover a large portion of the areola, not just the nipple. Her lips should be flanged out like a fish. You should not feel sharp nipple pain during feeding (initial discomfort for a few seconds is normal; sustained pain means the latch needs adjusting). Experiment with positions — cross-cradle, football hold, and side-lying all work. Get help from a lactation consultant if latch issues persist.
Newborn Jaundice
Jaundice is the yellowing of skin and eyes caused by elevated bilirubin — a byproduct of the normal breakdown of red blood cells. Newborns have many more red blood cells at birth than they need (the liver later processes the excess), and a newborn liver is not yet efficient at clearing bilirubin. Hence, jaundice.
Physiological Jaundice (Normal)
Appears on day 2–3, peaks around day 3–5, and usually resolves by about 2 weeks in full-term babies. The yellowing typically starts on the face and moves downward. Mild yellowing of face and upper chest with an otherwise feeding and active baby is usually physiological and self-resolving. Even so, have any newborn jaundice assessed by your pediatrician, because the level (not just the colour) determines whether treatment is needed.
When to Worry: Pathological Jaundice
Seek medical care the same day if:
- Jaundice appears within the first 24 hours of life (always pathological)
- The yellow color has spread to the abdomen or below the knees
- Your baby seems very sleepy, difficult to rouse for feeds, or refusing to feed
- The jaundice seems to be getting worse rather than better by day 5–7
- Baby is arching the back or high-pitched crying (signs of bilirubin toxicity)
Bilirubin Levels
Your pediatrician may order a transcutaneous bilirubin (TcB) measurement using a skin probe, or a serum bilirubin blood test. The threshold for treatment depends on age in hours and gestational age — not just a single number. This is why you should not interpret a number like “12 mg/dL” alone without context.
Sunlight: The Indian Tradition
Placing jaundiced babies in morning sunlight is an extremely common practice in Indian households, often guided by grandmothers. The science: sunlight does contain blue wavelengths that break down bilirubin in skin. However, the evidence for home sunlight exposure as a treatment for jaundice is limited — it is difficult to deliver a consistent therapeutic dose, there is a risk of sunburn, and overheating is dangerous. For mild, physiological jaundice in an otherwise well baby, brief indirect sunlight exposure (through a window, not direct outdoor sun) is not harmful and may provide a small benefit. But it is not a substitute for phototherapy when bilirubin levels are high. If your doctor says the baby needs phototherapy, sunlight at home is not an alternative.
Phototherapy
Hospital phototherapy uses specific blue-spectrum LED lights to break down bilirubin in the skin. It is safe, effective, and often works within 24–48 hours. Most babies can still be breastfed during phototherapy. Frequent feeding during phototherapy actually helps — more feeds mean more stool, and bilirubin is excreted through stool.
Cord Stump Care
The umbilical cord stump — the small, clamped remnant of the cord — dries and falls off on its own, usually between 7 and 21 days. It goes from yellow-green to brown to black and hard before detaching.
What to do:
- Keep it dry. Dry is the goal. Moisture delays separation and increases infection risk.
- Fold the front of the diaper down (or use newborn diapers with a notch) so the waistband sits below the stump.
- Expose to air when possible.
- Do not apply oil, turmeric, coconut oil, or any home remedies to the stump. These are common traditions in Indian households and are unfortunately harmful — they slow drying and introduce bacteria.
- In Indian hospital practice, a single application of chlorhexidine gel is sometimes recommended in the first days for infection prevention, particularly in home births or lower-resource settings. Follow your hospital’s or pediatrician’s specific guidance.
What is normal:
- A small amount of dried blood where it attaches to the skin
- Mild odor as it dries (not foul)
Signs of infection — seek care:
- Red, swollen, or warm skin spreading around the base of the stump
- Foul smell
- Discharge (pus or oozing)
- Baby seems unwell, not feeding, feverish
Do not try to remove the stump yourself even if it is “almost off.” Let it detach on its own.
Bathing a Newborn
Sponge Bath Until the Cord Falls
Until the cord stump falls off completely, only sponge baths. Immersing the baby in water before this slows cord drying and increases infection risk. A sponge bath means using a damp, warm cloth to wipe one area at a time while keeping the rest of the baby wrapped.
First Full Bath
Once the cord stump is gone, you can move to a full bath. Use a small baby tub or a clean plastic basin. The room should be warm — Indian homes in winter can be cold enough to chill a small baby quickly.
Water temperature: Around 37°C / 98–100°F. Test with your elbow or inner wrist, not your hand. It should feel warm but not hot.
How to bathe:
- Have everything ready before you undress the baby — towel, clean clothes, diaper.
- Support the head at all times. Your non-dominant arm goes under the baby’s back, hand supporting the head.
- Start with the face (eyes first, wiped outward), then head, then body front, then back.
- Genitals last — front to back for girls.
- Lift out, immediately wrap in a warm towel, and dry quickly including all skin folds.
How often: 2–3 times per week is sufficient for newborns. Daily bathing can dry out their skin.
Products: Tradition vs Evidence
Indian households often have established bathing rituals that vary by region. Here is an honest breakdown:
Besan (chickpea flour) baths: Used as a gentle scrub and cleanser, especially in the first weeks before the first full bath. Besan has mild surfactant properties. It is widely used but has no proven benefit; discuss with your pediatrician, and watch for any redness or rash. If you use it, make sure it does not go near the cord stump.
Soap: If you use soap, choose fragrance-free and specifically formulated for babies (pH-balanced). Adult soaps disrupt the skin barrier. Plain water is often sufficient for newborns.
Coconut oil as a moisturizer: Commonly used and does have some evidence for maintaining the skin barrier in newborns. Reasonable to use, particularly in dry climates.
Mustard oil on skin: A North Indian tradition. The evidence here is actually negative — mustard oil contains allyl isothiocyanate, which can damage the skin barrier in newborns and has been associated with skin reactions in studies from India. Best avoided on a newborn’s skin.
Baby Massage
Infant massage is perhaps the most universal tradition across Indian households — nani, dadi, the local dai, everyone has a view on how it should be done and with which oil.
What the Evidence Says
Infant massage is one of the better-studied complementary care practices. Research from AIIMS and international studies has found that regular massage:
- Promotes weight gain in low-birth-weight and preterm babies
- Improves sleep duration
- Reduces colic crying in some babies
- Supports bonding between caregiver and baby
- Stimulates circulation and muscle tone
It is a genuinely beneficial practice. The evidence is clearest for premature babies, but full-term babies benefit too.
When to Start
Wait until the cord stump has fallen off. For most babies, this means starting at 2–3 weeks. Begin with gentle strokes for 10–15 minutes once or twice a day, preferably before a bath (not immediately after a feed — wait at least 30–45 minutes).
Oil: Tradition vs Evidence
Sesame oil (til ka tel): The most studied oil in Indian newborn care research. Studies from the AIIMS group have shown that sesame oil massage is well-tolerated, does not damage the skin barrier, and may support weight gain in preterm infants. It is the most evidence-supported choice.
Coconut oil: Reasonable second choice. Does not damage the skin barrier. Evidence for massage benefits is thinner than sesame but used safely in many contexts.
Mustard oil (sarson ka tel): Widely used in North India but — as noted in the bath section — studies have found it damages the epidermal skin barrier in newborns. It is the most popular choice in tradition and one of the least supported by evidence. If your family uses it, the harm is primarily to the skin barrier rather than acute toxicity, but pediatricians now generally advise against it for newborns.
Olive oil: Commonly recommended in some Western parenting resources but evidence suggests it may impair the skin barrier in newborns more than sesame or coconut oil. Best avoided.
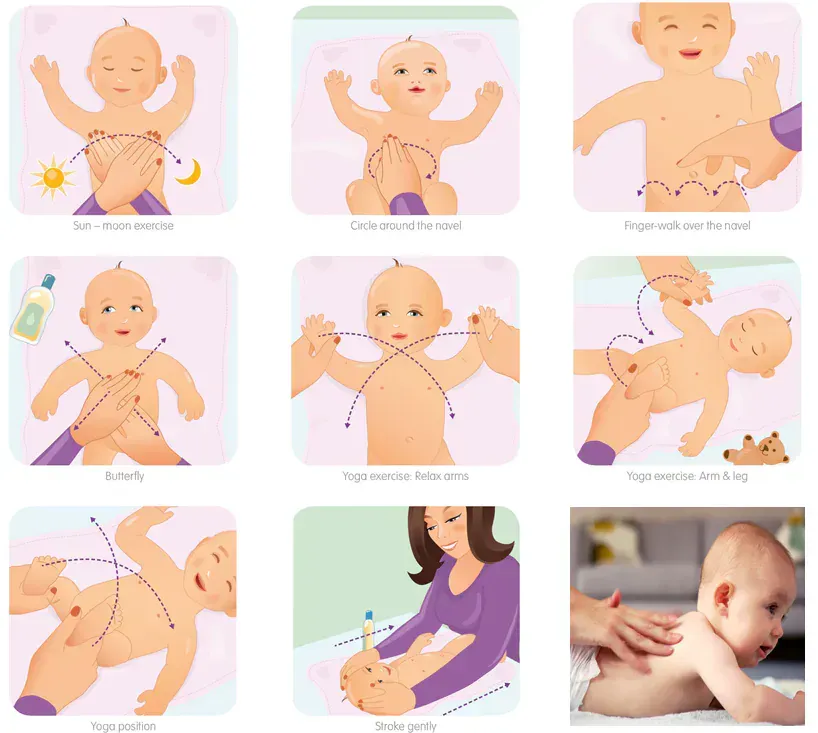
Technique
- Use warm oil (test on your wrist).
- Long, gentle strokes on limbs — from hip to ankle, shoulder to wrist.
- Clockwise circles on the abdomen (following the direction of bowel movement) — helps with gas.
- Gentle kneading on the back.
- Watch your baby’s cues — if she turns away, stiffens, or cries, stop. Not all babies enjoy massage from day one.
Sleep
How Much Newborns Sleep
A lot — and in a pattern that bears no resemblance to adult sleep. Newborns sleep 16–18 hours per day but rarely for more than 2–4 hours at a stretch. They do not yet have a circadian rhythm (that develops between 6–12 weeks). Night and day mean nothing to them. This is physiologically normal and not a problem to be solved in the first 4–6 weeks.
No Schedule in the First 4–6 Weeks
Every well-meaning relative will ask if the baby is “on a schedule” yet. The answer in the first 4–6 weeks should be: no, and that is correct. Attempting to impose a rigid schedule this early typically means missing hunger cues and risking inadequate feeding. Feed on demand. Sleep when the baby sleeps. Schedules become possible — and useful — from 3–4 months onward when the circadian rhythm begins to consolidate.
Safe Sleep: The Indian Reality
International guidelines recommend that babies sleep on their back, on a firm flat surface, in their own sleep space (a crib or bassinet), in the same room as the parents but not in the same bed. The AAP and IAP (Indian Academy of Pediatrics) both endorse this.
The reality in India is that bed-sharing (co-sleeping) is extremely common and culturally normalized — grandmothers co-slept, mothers co-slept, it is often seen as the natural way. Telling parents to “just don’t co-sleep” without addressing this reality is unhelpful.
If you are going to co-sleep (and many families will regardless of guidelines), the following significantly reduce the risk:
- Never on a sofa, armchair, or soft mattress — risk of suffocation is highest here
- Never after alcohol, sedating medication, or when extremely exhausted (where you cannot rouse on cues)
- Never with heavy blankets, duvets, or pillows near the baby’s face
- Keep the baby on the side furthest from the adult, or between the mother and the wall with a firm edge
- Baby on back, not stomach or side
- Do not swaddle tightly in a co-sleeping situation (baby needs to be able to move)
- No other siblings or pets in the same bed as the newborn
Breastfeeding reduces SIDS risk — the evidence for this is robust. Pacifier use also reduces SIDS risk, though it should be introduced only after breastfeeding is well-established (around 3–4 weeks).
Signs of safe sleep: Baby is on back, face uncovered, room not overheated, no loose bedding around face.
Crying and Soothing
Why Babies Cry
A newborn cries because it is her only language. The causes are not mysterious: hunger (the most common), discomfort (gas, wet diaper), tiredness, overstimulation, and — sometimes — no identifiable reason at all. In the first weeks, assume hunger first. Offer the breast. If the baby fed recently and is clearly not hungry, work through the checklist: diaper, temperature, gas, position.
The PURPLE Crying Period
The “Period of PURPLE Crying” is a recognized developmental phenomenon: a phase of peak crying that begins around 2 weeks, peaks around 6–8 weeks, and resolves by 3–4 months. The acronym describes it:
- Peak pattern (increases, then decreases)
- Unexpected — starts and stops for no clear reason
- Resists soothing
- Pain-like expression even when baby is not in pain
- Long bouts (lasting hours)
- Evening clustering (worse in late afternoon and evening)
This phase is normal and universal. It is the phase where parents are most at risk of overwhelming frustration. If you feel yourself losing control, put the baby down safely in the crib and walk away for a few minutes. Shaking a baby even once can cause permanent brain damage or death (shaken baby syndrome). This is not a moral failing — it is a physiological limit. Put the baby down and step out.
Colic
Colic is typically defined as crying for more than 3 hours per day, more than 3 days per week, for more than 3 weeks, in an otherwise healthy baby. It affects around 20% of babies. The cause is not definitively known — leading theories include gut immaturity, gas, and heightened neurological sensitivity. It is not caused by bad parenting or a poor diet (in breastfeeding mothers, dietary changes rarely help).
What helps (modestly): gas drops (simethicone), probiotics (Lactobacillus reuteri has the best evidence for breastfed babies), and the soothing techniques below. What does not help and is potentially harmful: gripe water (traditional Indian gripe water may contain alcohol, fennel, or sodium bicarbonate — none reliably effective, some harmful in newborns), herbal preparations.
Colic resolves on its own by 3–4 months in almost all cases. This is cold comfort at 2 AM, but it is real.
The 5 S’s
Harvey Karp’s “5 S’s” are a useful framework for soothing a distressed newborn:
- Swaddle — wrap snugly with arms at sides (hips loose — never swaddle the hips tightly, as tight hip swaddling causes developmental dysplasia of the hip). The Moro reflex is reduced when arms are contained.
- Side or stomach position — holding baby on her side or stomach in your arms for soothing (never for sleeping). This triggers the calming reflex.
- Shush — a continuous, loud white noise near the baby’s ear. Louder than you think — the womb was not quiet. A fan, vacuum cleaner sound, or white noise app works.
- Swing — gentle, rhythmic motion. Head-support is essential. Small, rapid jiggles (like you’re shaking a salad dressing) work better than big slow rocks.
- Suck — offering the breast, a clean finger, or a pacifier (once breastfeeding is established). Sucking activates the calming reflex.
Used together, they are effective for many crying newborns.
Diaper Changes
How Often
Newborns need 10–12 diaper changes per day on average. Do not let a wet or soiled diaper sit — newborn skin is thin and breaks down quickly.
What Is Normal in Urine
For the first 1–2 days, very few wet diapers is normal (the baby has received little fluid). By day 5, expect at least 6 wet diapers per day. Urine should be pale yellow. Orange or rust-colored spots in the diaper in the first day or two are urate crystals — usually harmless and very common. If they persist beyond day 3, mention to your pediatrician as they can signal dehydration.
What Is Normal in Stool
Meconium (days 1–2): Black, sticky, tar-like. This is the first stool, composed of amniotic fluid, skin cells, and bile. It is normal and expected. Delayed meconium passage (more than 24–48 hours) should be mentioned to your doctor as it can signal obstruction.
Transitional stool (days 2–4): Greenish-brown, less sticky. The gut is transitioning.
Milk stool (days 4–5 onward): For breastfed babies: yellow, seedy or mustardy, loosely formed, and — importantly — odorless or mildly sweet-smelling. Frequency varies widely: some breastfed babies go after every feed, others go once every few days. Both can be normal if the baby is otherwise comfortable.
Formula-fed babies produce brown, firmer, more formed stools that smell stronger.
Green stools: Occasionally normal. Persistently dark green or frothy stools in a breastfed baby may indicate foremilk-hindmilk imbalance (baby is getting too much foremilk). Mention to your pediatrician.
Diaper Rash Prevention and Treatment
The best prevention is keeping skin clean and dry. Change promptly after soiling. After cleaning, allow the skin to air-dry for 30–60 seconds before applying the diaper. A thin barrier cream (zinc oxide paste) at each change is effective for prevention and mild rash treatment. Do not use talcum powder — the particles are a respiratory hazard for babies.
For persistent or worsening rash (especially if there are satellite spots or the rash is in skin folds), suspect a yeast/fungal rash — which requires antifungal cream, not zinc oxide alone. See your pediatrician.
Common Newborn Concerns That Are Actually Normal
Hiccups
Frequent hiccups are normal in newborns. The diaphragm is immature and easily triggered. Hiccups do not bother babies the way they bother adults. No treatment needed.
Sneezing
Newborns sneeze frequently to clear their nasal passages — not because they have a cold. It is their only self-cleaning mechanism. Normal.
Noisy Breathing
Newborns breathe loudly, irregularly, and sometimes seem to make grunting sounds while asleep. Periodic breathing (short pauses of 5–10 seconds followed by rapid breaths) is normal in newborns. What is not normal: sustained grunting with each breath, ribs visibly pulling in with breathing (retractions), blue color around the lips, or noisy breathing that seems like effort. These are emergencies.
🚨 Call 112 (national emergency) or 108 (ambulance), or go to the nearest hospital, if you see: difficulty/noisy breathing; swelling of face/lips/tongue; widespread hives with vomiting; pale/grey/blue skin; floppiness/unresponsiveness; or a seizure. If an adrenaline auto-injector is prescribed, use it first, then go.
Spitting Up
Most newborns spit up. The valve between the esophagus and stomach is immature, and milk easily comes back up — especially after a full feed or when the baby is laid flat immediately after eating. This is reflux and is usually not a medical problem if the baby is gaining weight and otherwise comfortable. The condition is sometimes called “happy spitter.” Hold your baby upright for 20–30 minutes after a feed when possible. See a doctor if vomiting is forceful (projectile), blood-tinged, or the baby is losing weight.
Cradle Cap
Yellow, scaly patches on the scalp appearing in the first weeks. It looks concerning but is usually mild — it is essentially seborrheic dermatitis of infancy, related to maternal hormones. Gently massaging the scalp with coconut oil and then brushing away flakes with a soft brush helps. It resolves on its own by 3–6 months. Do not pick at the scales. See your pediatrician if the patches spread, become red and inflamed, weep, or look infected.
When to Call the Doctor Immediately
These are genuine red flags. Do not wait until morning. Do not try home remedies first. Go to your pediatrician or the nearest emergency immediately.
🚨 Call 112 (national emergency) or 108 (ambulance), or go to the nearest hospital, if you see: difficulty/noisy breathing; swelling of face/lips/tongue; widespread hives with vomiting; pale/grey/blue skin; floppiness/unresponsiveness; or a seizure. If an adrenaline auto-injector is prescribed, use it first, then go.
Call right now if your newborn has any of the following:
- ⚠️ In a baby under 3 months, ANY fever of 100.4°F (38°C) or higher is a medical emergency — see a doctor the same day, even at night. Do not give paracetamol and wait. Newborns cannot localize infection. A fever may be the only sign of a serious bacterial infection (meningitis, sepsis, UTI).
- Not feeding at all — Missing 2+ consecutive feeds in a baby who was previously feeding is not “just a tired phase.” It can signal infection, metabolic crisis, or jaundice toxicity.
- Jaundice reaching below the knees — or jaundice with a baby who is very sleepy and hard to wake.
- Seizures — jerking movements that are rhythmic and cannot be stopped by holding the limb, repeated eye deviation, or sustained body stiffening.
- Blue or dusky color around the lips (central cyanosis) — pale or gray color is equally alarming. This is not peripheral coldness (blue hands and feet are common and normal); it is color around the central mouth and tongue that matters.
- Bulging fontanelle — the soft spot at the top of the head should be slightly flat or mildly pulsatile. A bulging, tense fontanelle (when the baby is not crying) can indicate increased pressure in the brain.
- Sunken fontanelle — combined with dry mouth, no tears, fewer than 4 wet diapers in 24 hours — this is dehydration.
- Not urinating — fewer than 4 wet diapers in 24 hours after day 4 is a sign of inadequate fluid intake.
- Difficulty breathing — grunting, nostrils flaring, ribs pulling in, breathing faster than 60 breaths per minute at rest.
- Cord stump that is red, swollen, or oozing — with or without fever.
Postpartum Support: The Indian Family Context
The Joint Family as a Resource
Indian families have something that Western nuclear families genuinely lack: a built-in support system. Mothers, mothers-in-law, aunts, sisters — having experienced women around in the first weeks is invaluable. Tasks like cooking, cleaning, and older sibling care being handled by others gives the mother physical space to recover and breastfeed.
The tradition of a 40-day confinement period (the “chilla” or similar practices across cultures) exists for a reason: the mother’s body needs rest and nutrition to recover from birth and establish milk supply. This is not superstition — it is sound logic. Staying home, eating well, resting as much as possible, and focusing on feeding the baby is good medicine.
When Advice Conflicts
The same joint family that supports you may also offer advice that conflicts with what your pediatrician says — about mustard oil, about gripe water, about keeping the baby swaddled tightly all day, about giving water or honey. These traditions come from love and experience.
The approach that works: frame it as what has changed. “The research has found that…” or “The doctor asked us specifically not to…” is easier than “That’s wrong.” Pick your battles — a little besan bath is unlikely to harm your baby; a spoon of honey (botulism risk) or tight hip swaddling (developmental dysplasia risk) is something to firmly but kindly push back on.
When the Mother Needs Help
Watch for the new mother too. Baby blues — tearfulness, mood swings, exhaustion — in the first 1–2 weeks is extremely common and usually self-resolving. Postpartum depression is different: persistent sadness, inability to bond with the baby, feeling like a bad mother, withdrawing from the baby, intrusive scary thoughts. It affects 10–15% of mothers and is treatable. It is not weakness. If this describes someone in your family, help her reach a doctor. She should not white-knuckle it alone.
Frequently Asked Questions
Q: My newborn is sleeping all day and only waking once or twice at night. Should I wake her to feed?
Yes, in the first 2 weeks, absolutely. A newborn who is too sleepy to demand feeds may not be getting enough nutrition and may have elevated jaundice that is making her sleepier. Wake her every 3 hours to feed until your pediatrician confirms weight gain is on track.
Q: Can I give my baby water in the summer?
No. Exclusively breastfed or formula-fed babies under 6 months should not receive water. Breast milk is 88% water and provides adequate hydration even in Indian summers. Extra water in newborns can cause a dangerous condition called hyponatremia (low sodium in the blood). This is one of those traditions to firmly decline.
Q: When should the first pediatrician visit happen after hospital discharge?
Within 2–5 days of discharge for most newborns, or as directed by your hospital. The key things checked at this visit: weight, jaundice, feeding, cord stump, and any concerns from the hospital stay. Do not skip this visit even if “the baby looks fine.”
Q: My mother-in-law wants to give the baby ghee or honey in the first days. Is that okay?
Honey is a firm no before 12 months — it can contain Clostridium botulinum spores that a newborn’s gut cannot protect against, causing infant botulism, which can be fatal. Ghee in the first days before feeding is established has no benefit and may interfere with the baby’s desire to breastfeed. Both can wait.
Q: How do I know if my baby is too hot or too cold?
Feel the back of the neck or the chest — these are better indicators than hands or feet, which are often cool in newborns. The chest and neck should feel warm and comfortable, not sweaty or cold. A useful rule: dress your newborn in one more layer than you are wearing comfortably. In Indian winters, that means warm inner layer plus a blanket when stationary. Overheating is an independent risk factor for SIDS.
Q: When do newborns start to smile?
A real, social smile — in response to your face — typically appears anywhere in the 6–8 week range, and some healthy babies take a little longer. Before that, you may see reflex smiles during sleep, but the first real “I see you and I’m happy” smile is one of the most rewarding moments of the fourth trimester. It signals that the social brain is coming online. Red flag: if your baby is not smiling socially by 3 months, mention it to your pediatrician — it is often nothing, but it is worth a developmental check.
This guide is reviewed by Babynama Pediatricians. It is not a substitute for direct medical advice from your child’s doctor. If you have concerns about your newborn’s health, consult a pediatrician promptly.
Real Questions from Indian Mothers
These are real questions asked by parents in the Babynama community, answered by our pediatricians.
“My baby is 1.5 months old and since when he has got his vaccination he is kinda reckless, doesn’t relax like before vaccination. Mostly cranky and crying. He had colic issue 3-4 days but now he is better but still cranky. What could be the reason?”
Some crankiness can happen after vaccination. Apply a cloth-wrapped ice pack at the injection site and distract the baby. At 1.5 months (under 3 months), do not give paracetamol on your own — any fever of 100.4°F (38°C) or higher at this age is a medical emergency and needs to be seen by a doctor the same day, who will decide on paracetamol and the exact dose. Paracetamol is dosed by your baby’s weight, not age: 15 mg/kg per dose, every 4–6 hours, max 4 doses (60 mg/kg) in 24 hours — but not for under-3-months without a doctor. Confirm the exact mL with your pediatrician.
“Baby does not cry much because of colic but the amount of gas that comes out has increased, that’s why wanted to know if it is because of the formula or anything else”
Okay! Try Burping the baby well. Give tummy massage. Do cyclic moments of legs. Give tummy time. If not resolved, then we will plan regarding formula milk if symptoms doesn’t improve
“Good evening docs, baby have been started on solids approx 3 weeks.. initially, it was good.. since 2 days his stool is very hard.. He’s being given fruit purees and dal chawal with veggies.. what am I doing wrong?”
Constipation is very common after starting solids. (Note: solids and water are only for babies 6 months and older — nothing other than breast milk or formula before 6 months.) You can give ripe papaya, pears, or peaches, offer some water with meals, include fibre-rich foods, and do daily tummy massage and leg cycling. If the stool stays very hard, there is blood, or your baby seems in pain or is not passing stool, see your pediatrician.
General information for Indian parents, not a substitute for your pediatrician. In an emergency, call 112 or 108.