Quick Answer
Cyclic Vomiting Syndrome (CVS) is frightening to witness, but it is usually manageable and most children outgrow it. If your child has episodes of severe, repeated vomiting that come and go with symptom-free periods in between, they may have CVS. While scary during episodes, CVS is not generally associated with lasting damage, and with proper management episodes can often be reduced or prevented. The main risk during an episode is dehydration, which sometimes needs hospital care, so always watch for the red flags below. You’re not alone - this guide helps you understand and manage your bachcha’s CVS.
What Is Cyclic Vomiting Syndrome? (CVS Kya Hai)
Understanding CVS
CVS is a pattern of:
-
Severe, repeated vomiting episodes
-
Episodes last hours to days
-
Symptom-free, back to their usual self between episodes
-
No other cause found (not infection, obstruction, etc.) Key features:
-
Episodes are predictable (same pattern each time)
-
May be triggered by specific factors
-
Often related to migraines
-
Usually starts between ages 3-7
The Episode Cycle
Four phases:
| Phase | What Happens | Duration |
|---|---|---|
| Prodrome | Early warning signs (nausea, pallor, sweating) | Minutes to hours |
| Vomiting | Intense, repeated vomiting (6-12 times/hour) | Hours to days |
| Recovery | Vomiting stops, appetite returns slowly | Hours to days |
| Well interval | Symptom-free, back to usual self | Days to months |
Signs and Symptoms (Lakshan)
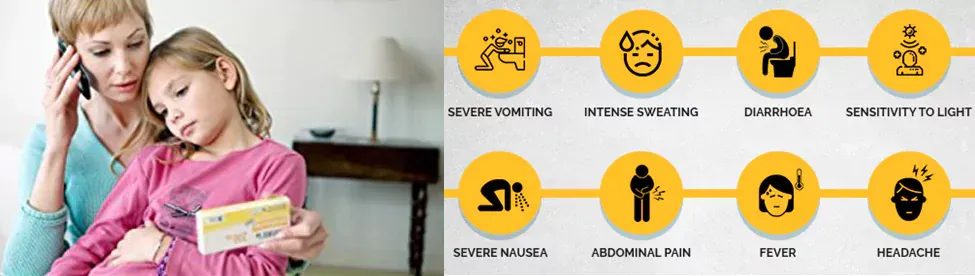
During an Episode
Main symptoms:
-
Severe, forceful vomiting
-
Vomiting 6+ times per hour at peak
-
Pale, sweaty skin
-
Extreme fatigue/lethargy
-
Stomach pain
-
Loss of appetite
-
Sensitivity to light and sound
-
Headache
-
Low-grade fever (sometimes)
-
Drooling or spitting Each episode:
-
Starts similarly (child may recognize warning signs)
-
Follows same pattern
-
Lasts about the same time
Between Episodes
Usually symptom-free
- No symptoms
- Normal eating
- Normal activity
- Normal energy
What Causes CVS?
The Connection to Migraines
Important: Up to 80% of CVS children have family history of migraines!
- CVS is considered a “migraine variant”
- Same brain pathways involved
- Similar triggers
- Many children develop migraines later
Common Triggers
| Category | Specific Triggers |
|---|---|
| Emotional | Excitement, anxiety, stress, anticipation |
| Physical | Exhaustion, illness, lack of sleep (neend ki kami) |
| Food | Chocolate, cheese, MSG, caffeine |
| Other | Travel, motion sickness, fasting, periods (in older girls) |
Learning your child’s triggers is KEY to prevention!
When to Worry (Red Flags)
🚨 Call 112 (national emergency) or 108 (ambulance), or go to the nearest hospital, if your child:
- Is very drowsy, hard to wake, confused, or floppy
- Has signs of severe dehydration (no urine for 6+ hours, very dry mouth, sunken eyes, no tears)
- Is vomiting blood, or vomiting green/yellow bile
- Has severe, constant abdominal pain
- Cannot keep down even small sips of fluid
Seek same-day medical care if:
-
First episode ever (need to rule out other causes)
-
Episode is longer or different than usual
-
Child looks more unwell than in previous episodes Call doctor during episode if:
-
Child looks very ill
-
Episode differs from usual pattern
-
Vomiting blood or bile
-
Signs of dehydration
Diagnosis
CVS is diagnosed by:
-
Pattern of episodes (Rome criteria)
-
At least 3 episodes in 6 months
-
Normal between episodes
-
No other cause found Tests to rule out other causes:
-
Blood tests
-
Urine tests
-
Imaging (ultrasound, CT if needed)
-
Upper GI study
-
Possibly endoscopy
What You Can Do (Ghar Pe Kya Karein)
Identify and Avoid Triggers
Keep a diary of:
-
What child ate before episode
-
Sleep pattern (kitni neend li)
-
Stress/excitement level
-
Any illness before
-
Physical activity
-
Travel or events Common preventable triggers:
-
Ensure regular, adequate sleep
-
Don’t skip meals
-
Avoid known food triggers
-
Manage stress and anxiety
-
Treat infections promptly
Managing an Episode at Home
Early phase (prodrome):
-
If you recognize early signs, EARLY intervention helps!
-
Dark, quiet room
-
Anti-nausea medication (if prescribed)
-
Sometimes stopping the episode is possible if caught early During vomiting phase:
-
Quiet, dark room
-
Don’t force food or drink
-
Small sips of water or ORS (Electral / WHO-ORS) if tolerated
-
Cool cloth on forehead
-
Prescribed medications
-
Monitor for dehydration Recovery phase:
-
Gradual return to eating
-
Start with clear fluids
-
Progress to bland foods (khichdi, toast, banana)
-
Rest
-
Don’t rush normal activity
Preventing Dehydration
Signs of dehydration:
-
Decreased urination (less than 3-4 times/day)
-
Dark urine
-
Dry mouth and lips
-
No tears when crying
-
Sunken eyes
-
Lethargy If dehydrating:
-
May need IV fluids
-
Don’t hesitate to go to hospital
Treatment Options
Preventive Medications
For frequent episodes, doctor may prescribe:
- Cyproheptadine (common in younger children)
- Amitriptyline
- Propranolol
- Others based on individual needs Goal: Reduce frequency and severity of episodes
Treatment During Episodes
| Medication Type | Purpose |
|---|---|
| Anti-nausea (ondansetron) | Stop vomiting |
| Sedatives | Help child sleep through episode |
| IV fluids | Prevent dehydration |
| Pain medication | For headache/abdominal pain |
Lifestyle Measures
- Regular sleep schedule
- Regular meals (no fasting)
- Stress management
- Avoid known triggers
- Coenzyme Q10 supplements (sometimes recommended)
Prognosis (Kya Hoga Aage)
Good news:
- Most children outgrow CVS by puberty
- Episodes typically decrease with age
- Quality of life between episodes is normal
- Treatment helps reduce episodes Note: About 75% develop migraines later in life
Coping Strategies for Parents
During Episodes
- Stay calm (your stress affects child)
- Trust the process if pattern is known
- Have action plan ready
- Know when to seek help
Between Episodes
- Focus on normal life
- Don’t overly restrict child
- Work on trigger prevention
- Connect with other CVS families
School Management
- Inform school about condition
- Provide action plan
- May need flexible attendance policy
- Teacher should recognize warning signs
Frequently Asked Questions
Q: Bachche ko baar baar ulti ho rahi hai, kaise pata chalega CVS hai?
A: CVS pattern: severe vomiting episodes that start and end suddenly, last hours to days, then symptom-free and back to usual in between. Episodes are similar each time. Must have 3+ episodes in 6 months with no other cause. Doctor will do tests to rule out infection, obstruction, etc. If pattern matches and tests normal - likely CVS. Don’t self-diagnose - see specialist.
Q: Episode ke time kya khilana chahiye?
A: During active vomiting: nothing! Don’t force food or drink - it won’t stay down and causes more vomiting. Once vomiting slows: small sips of water or ORS (Electral / WHO-ORS). Recovery: start with bland foods - khichdi, plain rice, toast, banana. Gradually return to normal diet. Force-feeding during episode makes things worse.
Q: CVS theek ho sakta hai?
A: Most children OUTGROW CVS by puberty! While there’s no “cure,” preventive medicines can reduce episodes significantly. Identifying and avoiding triggers helps. As child grows, episodes typically become less frequent and less severe. Many children are episode-free by teenage years (though may develop migraines later).
Q: Hospital le jaana padega har baar?
A: Not always, once you know the pattern. Mild episodes may be managed at home with rest, darkness, prescribed medications. BUT go to hospital if: first ever episode, severe dehydration, blood in vomit, can’t keep any fluids down, episode longer/different than usual, or child looks very sick. When in doubt, seek medical care.
Q: Stress se CVS hota hai?
A: Stress is a common TRIGGER, not the cause. Both emotional stress AND excitement can trigger episodes. Other triggers: lack of sleep (neend ki kami), skipping meals, certain foods, infections. The underlying cause is likely related to migraine pathways in brain. Managing stress helps prevent episodes but stress alone doesn’t cause CVS.
This article was reviewed by Babynama Pediatricians. Last updated: June 2026
Child has CVS or repeated vomiting episodes? Babynama’s pediatricians can help with management plans and support. Chat with us on WhatsApp!
Need personalized guidance? Book a consultation with our pediatricians or explore our Care Plans for 24/7 expert support!
Disclaimer: This article is for general informational purposes for parents in India and is not a substitute for professional medical advice. CVS is diagnosed and managed by a pediatrician or pediatric gastroenterologist — preventive and anti-nausea medicines must be prescribed and dosed by your treating doctor. Always consult your pediatrician for advice specific to your child. In an emergency, call 112 (national emergency) or 108 (ambulance), or go to your nearest hospital.
Have a question about your little one?
Join our free community for live Q&A with MD pediatricians — no cost to join.
Join the free community