Quick Answer
If your baby boy has been diagnosed with hypospadias, please know that this is a common and treatable condition! Hypospadias occurs in about 1 in 250-300 baby boys. It means the urethral opening (where urine comes out) is not at the tip of the penis but somewhere along the shaft. Surgery can successfully correct this, and most boys go on to have good urinary and sexual function.

Understanding Hypospadias
What is Hypospadias?
- Birth defect affecting the penis
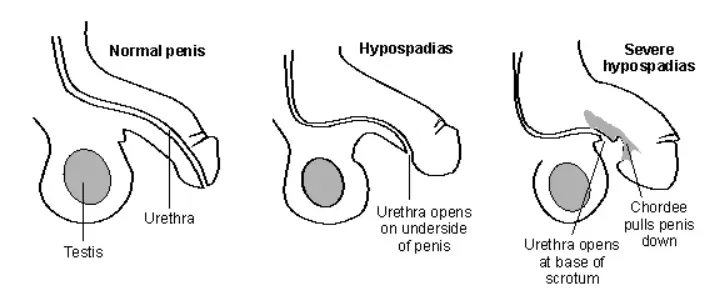
- Urethral opening (meatus) is in wrong position
- Not at the tip, but somewhere along shaft or scrotum
- Occurs during fetal development (9-12 weeks pregnancy)
- Very common - you’re not alone! Types Based on Location:
| Type | Location | Severity |
|---|---|---|
| Distal/Glanular | Near tip of penis | Mild (most common - 70%) |
| Midshaft | Along middle of penis | Moderate |
| Proximal/Penoscrotal | Near base of penis/scrotum | More severe |
Why This Happens
Causes (Usually Unknown):
-
Exact cause unclear in most cases
-
Development issue during weeks 9-12 of pregnancy
-
Genetic factors may play role
-
May run in families
-
NOT caused by anything you did during pregnancy! Risk Factors:
-
Family history of hypospadias
-
Older mother (35+)
-
Maternal obesity
-
Certain fertility treatments
-
Environmental factors (rarely proven) Important: In most cases, no specific cause is found. Don’t blame yourself!
What You May Notice
Signs of Hypospadias:
-
Urethral opening not at tip of penis
-
“Hooded” foreskin (skin only on top, incomplete underneath)
-
Downward curve of penis (chordee)
-
Abnormal spray when urinating
-
May need to sit to urinate (if severe) Usually Noticed:
-
At birth during examination
-
During newborn checkup
-
Sometimes missed until diaper changes
When to Worry (Red Flags)
Contact your pediatrician/urologist if:
-
Difficulty urinating
-
Pain during urination
-
Infection signs (fever, redness, swelling)
-
Concerns about appearance
-
Questions about treatment timing Important Notes:
-
Do NOT circumcise before consulting urologist
-
Foreskin may be needed for surgical repair
-
Discuss with pediatric urologist first
Treatment: What to Expect
Surgery is the Standard Treatment:
| Aspect | Details |
|---|---|
| Age for Surgery | Usually 6-18 months (ideal: 6-12 months) |
| Type | Usually single surgery, sometimes staged |
| Duration | 1-3 hours depending on severity |
| Hospital Stay | Often same-day or overnight |
| Recovery | 2-4 weeks, full healing in 6 months |
Goals of Surgery:
-
Place urethral opening at tip of penis
-
Straighten any curve (chordee)
-
Create normal appearance
-
Allow normal urination standing up
-
Ensure future sexual function Before Surgery:
-
No circumcision (foreskin used for repair)
-
Regular pediatric urologist visits
-
Plan timing around family schedule
-
Prepare for post-operative care
Post-Surgery Care
Immediately After:
-
Catheter may be in place (usually 1-2 weeks)
-
Dressing/bandage on penis
-
Pain medication as needed
-
Avoid straddling toys (no car seats for prolonged time) Wound Care:
-
Keep area clean and dry
-
Change diaper frequently
-
Watch for signs of infection
-
Follow specific surgeon instructions What to Expect:
-
Swelling and bruising (normal)
-
Some bloody drainage (normal)
-
Child may be fussy initially
-
Healing takes several weeks Concerning Signs (Call Doctor):
-
Any fever in a baby under 3 months (≥100.4°F / 38°C) is a same-day emergency — see a doctor immediately, do not medicate and wait at home
-
Fever ≥38.5°C in an older baby
-
Heavy bleeding
-
Unable to urinate (no urine for several hours)
-
Severe pain not relieved by medication
-
Signs of infection (pus, increasing redness)
🚨 If your baby has heavy uncontrolled bleeding, will not wake/respond, or struggles to breathe, call 112 (national emergency) or 108 (ambulance), or go to the nearest hospital.
For pain or fever after surgery, give paracetamol only as prescribed by your surgeon — it is dosed by weight (about 15 mg/kg/dose, every 4–6 hours, maximum 60 mg/kg/day). Check your syrup’s strength before measuring. Do not give paracetamol to a baby under 3 months without a doctor’s advice.
What You Can Do
Before Surgery:
-
Find experienced pediatric urologist
-
Ask questions about their experience
-
Understand the procedure
-
Plan for recovery time at home
-
Arrange help for post-op period Emotionally:
-
Know this is common and treatable
-
Outcomes are generally excellent
-
Your son will likely have normal function
-
Connect with other parents if helpful
-
Don’t feel guilty - this isn’t anyone’s fault Practical:
-
Document doctor’s instructions
-
Prepare home for recovery
-
Stock up on diapers and soft clothing
-
Plan for time off work if needed
Long-Term Outcomes
Good News:
-
Surgery success rate is high (90%+)
-
Most boys have normal urination
-
Sexual function usually normal
-
Fertility usually unaffected
-
Cosmetic results generally good Possible Complications (Uncommon):
-
Fistula (extra opening) - may need minor repair
-
Stricture (narrowing) - may need follow-up
-
Some may need second surgery
-
Regular follow-up recommended
Frequently Asked Questions
Q: Doctor ne bola hai ki baby ka operation hoga - kya yeh safe hai?
A: Yes, hypospadias surgery is very safe when done by an experienced pediatric urologist. It’s one of the most common pediatric urological surgeries. The techniques have improved significantly over decades. Complications are uncommon, and most boys have excellent outcomes with normal function.
Q: Why didn’t they do circumcision at birth like other babies?
A: In hypospadias, the foreskin is often incomplete (looks “hooded”). More importantly, the foreskin tissue is valuable for surgical repair - surgeons use it to reconstruct the urethra. Circumcising would remove tissue needed for surgery. Always consult the urologist before any decision about circumcision.
Q: Will my son have normal sexual function as an adult?
A: Yes, in the vast majority of cases! When surgery is done properly, boys grow up to have normal sexual function and fertility. The goal of surgery is to ensure normal appearance and function. Most men with repaired hypospadias have normal intimate lives and can father children.
Q: At what age should surgery be done?
A: Most pediatric urologists recommend surgery between 6-18 months of age. This timing is ideal because: healing is faster in young babies, child won’t remember the surgery, and psychological impact is minimized. Earlier surgery also completes treatment before potty training age. Your surgeon will recommend best timing for your child.
Q: Kya yeh condition next baby mein bhi ho sakti hai?
A: There is a slightly higher risk if one child has hypospadias. If one son is affected, the risk for the next male child is about 10-15% (compared to 0.3% in general population). If the father had hypospadias, risk is about 8%. However, most subsequent male babies will NOT have it. Talk to a genetic counselor if you’re planning another pregnancy.
This article was reviewed by a pediatrician. Last updated: January 2025
Need personalized guidance? Book a consultation with our pediatricians or explore our Care Plans for 24/7 expert support!
General information for Indian parents, not a substitute for your pediatrician. In an emergency, call 112 or 108.
Have a question about your little one?
Join our free community for live Q&A with MD pediatricians — no cost to join.
Join the free community